
Dr. Philip McMillan, John McMillan
Ask most people about COVID today and you will get a shrug. The word itself has become something nobody wants to hear. Search traffic has fallen off a cliff, much of the scientific community has turned its attention elsewhere, and the public has decided, reasonably enough, that it would rather move on. That collective exhale is exactly the problem. Falling attention does not mean the danger has left the building. It may mean the danger is now free to grow in the dark.
The data that almost no one is reading tells a story that does not match the one the world settled on in 2020. Across age groups, the post-pandemic numbers are moving in worrying directions. Cirrhosis of the liver has climbed by close to 100 percent. Toxic liver disease is rising. Children are turning up with liver abnormalities. In adults between 18 and 29, disorders of mineral metabolism and liver problems lead the list. Move into the 45 to 59 bracket and the standout is hypertensive heart and renal disease. Something is off, and the puzzle is how few people seem to want to know why.
Same Virus, Different Disease
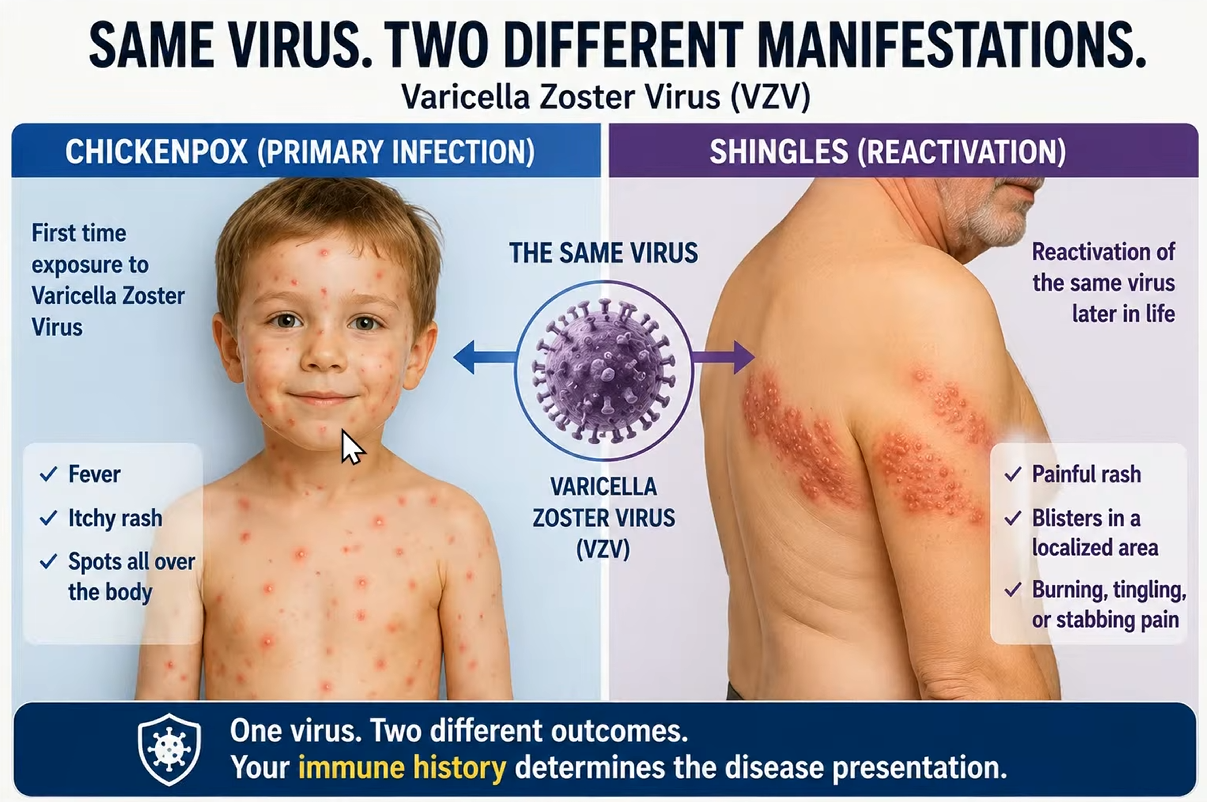
Start with a virus most parents already know. Varicella zoster gives small children chickenpox: fever, an itchy rash, spots everywhere. The same virus, reactivating decades later in an older adult, produces shingles, a different illness entirely. If you did not know they shared a cause, you would take them for two separate diseases.
COVID now behaves the same way. The version that filled hospitals early in the pandemic was mainly a respiratory illness, marked by inflammation of the heart, blood clots, and neurological symptoms. That is the picture seared into public memory. What is showing up now looks different. The damage is longer and more chronic: multi-organ impact, systemic disease, abnormal patterns scattered across different organs. A highly immune-evasive variant of the virus is here, but it is no longer announcing itself the way it once did. People keep watching for the old fire and miss a slower burn.
The COVID Storm
The principle worth holding onto is simple: do not underestimate reinfection. Prior infection, prior vaccination, then another exposure, and the disease can present in a different form. It has a name, the COVID storm, and it is not really a story about the virus at all. It is a story about the immune system.
The trigger is spike protein reaching the bloodstream in someone whose immune system is already primed to overreact. As Dr. Philip McMillan, a British clinician and researcher puts it, “It’s not the virus. It’s the immune system targeting virally infected cells being triggered with autoimmune responses that runs into this risk of causing organ damage.” If that holds, it changes who we should be paying attention to.
Who Is at Risk
Three groups stand out. The first is the most obvious: people who had severe or moderate-to-severe COVID, the ones who were hospitalized and survived. Their immune systems are already primed by that experience, having mounted one hyperimmune response. This is the group that warranted the most caution, because they had already been through a natural version of the reaction that does the harm.
The second group is the vaccine hyper-responder: people who reacted strongly after vaccination, with hypermetabolic lymphadenopathy, swollen lymph nodes, immune symptoms persisting past the normal window. That prolonged reaction is itself a signal, possible evidence that the systemic immune system has been primed and is quick to fire.
The third group is primed in the same systemic way but carries a second vulnerability: their mucosal immunity, the body’s frontline barrier, does not hold. They catch reinfection after reinfection because the first line of defense keeps failing. Once the system is primed, every breach becomes a chance for the storm.
The Castle and the Fence
Picture strong mucosal immunity as a castle. The walls are up, the artillery is mounted, there is a gate and a moat. A virus arriving at those defenses struggles to get inside. Even someone who once had severe COVID, if they are left with strong mucosal immunity, stays largely protected, because the real damage only happens once the enemy is through the gates.
Now picture weak mucosal immunity. The wall has been replaced by a flimsy fence. To compensate, the grounds are packed with soldiers, which is what systemic immune priming effectively does. Plenty of antibodies, plenty of immune cells, all stationed inside. When the virus slips past the fence, the fighting happens within your own walls. The soldiers do their job, and in doing it they damage the very thing they are defending.
This is the part that gets missed. Most of the serious harm in severe COVID and beyond comes from the immune response, not the pathogen. The body’s own defenses, triggered into autoimmune overdrive against infected cells, can end up damaging organs. The old vaccinated-versus-unvaccinated argument misses the point. The question that matters is whether someone is mounting systemic responses to spike protein that has reached the bloodstream. The tells are recognizable: feeling unwell for longer, a longer list of symptoms, blood pressure drifting off, a wave of gut and intestinal trouble. Each one suggests the virus got past the wall.
Reading the Damage by Age
The pathology lines up with the theory. In the 45 to 59 cohort, blood pressure and kidney function are the markers going wrong. Move to ages 60 to 74 and myocarditis appears, a sign the virus has reached the heart. In the very oldest group, the most striking figure: a 300 percent increase in myocarditis. Read together, these point in one direction, toward damage happening inside the castle rather than at its walls.
Some signals are openly speculative, offered as instinct rather than proof. A recent viral outbreak on a cruise ship may have been preceded by a wave of COVID. An athlete who fell ill had a sinus infection two weeks earlier, plausibly some form of COVID presentation. There are no hard facts on either, only the questions worth asking, and almost no one is asking them.
No Moving On
So why the silence? Part of it is exhaustion; the public is tired and wants the chapter closed. Part of it runs deeper. To seriously question COVID now means revisiting decisions made during the pandemic, and few in science are eager to return to that ground. The result is a quiet truce between a weary public and an uncomfortable scientific community. The implications do not move on with us. The organ damage keeps accruing whether or not anyone is watching.
Dr. McMillan’s assessment is stark: “We need answers. We need them now. We need them quickly. But sadly, we may have been gone past the point of mitigation.” Whether the data ultimately bears it out remains an open question. What is harder to dispute is that the signal deserves a look.


I am still listening for the outcomes
A fourth group perhaps? From Drs. McMillan and Chetty I learned about mast cell degranulation. More recently from Drs. Campbell and Peers, I was introduced to MCAS (and Augmented NAC). Their references took me to a 2016 lecture by Dr. Lawrence Afrin on MCAS. All my numerous Vax Injury symptoms can by explained by it, and seem to be helped by using an H1 and an H2 over-the-counter anti-histamines. I know I my case is only N=1, but I think it is worth consideration.