
Dr. Philip McMillan, John McMillan
A new study out of Toronto was supposed to close the book on one of the most contentious questions in post-pandemic medicine: do COVID-19 vaccines increase the risk of sudden cardiac death in young, healthy adults? The answer, according to the researchers, is no. But the data they collected tells a more complicated story, one that deserves far more attention than the headline received.
The case-control study, published in 2026, drew from a population of roughly six million people in Ontario, Canada. Researchers identified 4,806 individuals aged 12 to 50 who experienced sudden death between April 2021 and June 2023, then matched them against 24,030 living controls. They excluded anyone with documented comorbidities, aiming to isolate the effect of vaccination on otherwise healthy people. Their conclusion was unambiguous: “These findings do not support the hypothesis that COVID-19 vaccines increase the risk of sudden cardiac deaths in young healthy adults.”
For many, that settled it. But Dr. Philip McMillan, a physician and researcher who has spent years tracking post-pandemic cardiovascular trends, argues the paper reveals something its authors did not pursue. “You cannot explain to me pathophysiologically how that can be protective to the heart,” he said. “I can acknowledge that okay maybe the risk is really tiny but from my perspective, if you show me protection, I think there is something wrong with your data.”
The Numbers That Don’t Add Up
He is referring to the study’s odds ratios. Across every vaccination cohort, the numbers did not simply show no increased risk. They showed what appeared to be a protective effect. At least two doses of COVID vaccination carried an odds ratio of 0.53 for sudden death. Any mRNA vaccination came in at 0.57. Any COVID vaccination at all registered 0.63. These figures place vaccination squarely on the protective side of the ledger, well to the left of the neutral 1.0 mark.
On the surface, that sounds like good news. But consider the biology. COVID vaccines, particularly mRNA vaccines, carry a recognized risk of myocarditis, especially in younger males. Research has shown that cardiac glucose and fat metabolism can remain altered for up to 180 days following vaccination. These are not trivial effects. They represent documented, measurable changes to how the heart functions.
So how does something that can damage the heart also protect it from sudden death? McMillan uses a blunt analogy. If a study emerged showing that smoking was protective against lung cancer, no reasonable person would celebrate and encourage the population to light up. They would go back to the data and look for what went wrong. The same logic, he argues, applies here.
One detail in the paper stands out as particularly telling. While recipients of two or more vaccine doses showed an odds ratio of 0.53, those who received only a single dose came in at 0.88. If vaccines genuinely protect the heart, why would one dose offer so much less protection than two? The gap is difficult to explain through a protective mechanism. It is easier to explain through confounding. The unvaccinated accounted for 32.6 percent of sudden death cases but only 22.9 percent of controls, a disproportion that may reflect differences in health-seeking behavior, access to care, or other unmeasured variables rather than a true biological effect of vaccination.
The COVID Storm Hypothesis
But the most striking finding may be one the authors did not explore further. Among those who died suddenly, 2.2 percent had tested positive for COVID-19 within the previous 90 days. Among living controls, that figure was just 0.9 percent. The recently infected were dying at more than double the rate. McMillan sees this as the strongest signal in the entire paper, and it aligns precisely with a model he has been developing for years: the COVID storm.
The concept works like epoxy. One component alone does not trigger the reaction. Immune priming, whether from vaccination or a severe prior infection, creates a state of cardiac vulnerability. For most people, this vulnerability may remain silent. But when a subsequent SARS-CoV-2 infection arrives, the immune system responds in a way that targets already-sensitized cardiac tissue. The result is what McMillan describes as a spike-triggered autoimmune response: chest pain, palpitations, shortness of breath, reduced exercise tolerance, and in the worst cases, sudden cardiac events.
“The two are like epoxy. One or the other doesn’t actually cause anything to happen but when you put them together you get this COVID storm,” McMillan explained. “This is now like a new disease.”
A Population-Level Pattern
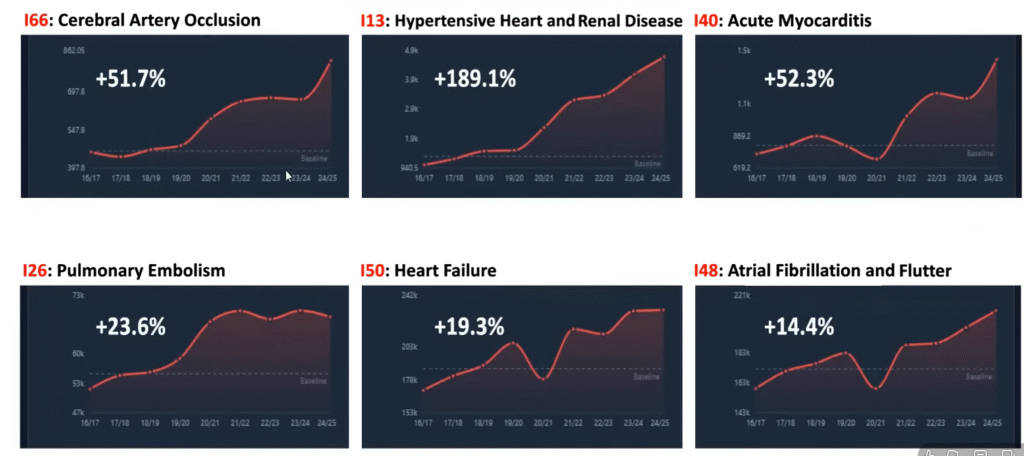
The population-level data supports this concern. An analysis of 186 million hospital episodes in the United Kingdom reveals a disturbing pattern of rising cardiovascular conditions since 2020-2021. Cerebral arterial occlusion is up 50 percent. Hypertensive heart and renal disease has surged 189 percent. Myocarditis has climbed 50 percent. Pulmonary embolism, heart failure, and atrial fibrillation are all trending upward across multiple ICD diagnostic codes. These are not marginal shifts. They represent a broad, sustained increase in cardiac disease across the population, and no one has identified the mechanism.
The Toronto study had an opportunity to probe deeper. Of the 107 individuals who died suddenly after a recent COVID infection, their vaccination status was not reported. That single cross-tabulation, how many of the recently infected who died had been vaccinated, and with how many doses, could have tested the COVID storm hypothesis directly. Its absence is a significant missed opportunity.
Where Research Must Go Next
McMillan argues that future research must move beyond binary framing. The question is not simply whether vaccines are safe or dangerous. It is whether a specific subset of the population, those who experienced cardiac symptoms following vaccination or severe infection, face compounding risk with each subsequent SARS-CoV-2 exposure. Identifying this cohort and understanding their trajectory is not an academic exercise. It is a clinical imperative.
The study also excluded individuals with comorbidities. A parallel analysis including that group might reveal whether immune-primed individuals with pre-existing cardiac vulnerabilities face an even steeper risk curve. The raw data, if made available for independent analysis, could answer questions the original researchers did not think to ask.
The cardiovascular trends are not going away. Cardiac conditions continue to climb across populations worldwide, and the pace shows no sign of slowing. Whether the mechanism is infection alone, immune priming alone, or the collision of the two, the data is demanding an answer. The only truly dangerous position is the one that refuses to look.


This all seems to be very consistent with the first things I heard about myocarditis when I first heard about it in 2021, ie., that any doctor speaking about this condition would be saying that once someone had it, they would expect 50% to be dead within 5 years.
Strange how you use “Toronto Study” and not specify the authors and perhaps where it was published (what “journal, etc.)